Kidney stones are a common presentation to the emergency department and GPs. Usually it is felt as a dull pain on one side of the lower back. If it falls into the ureter (the fine tube that drains urine from the kidney to the bladder) very severe pain that radiates into the groin, testes or labia can be experienced. It is a colic as the pain comes in waves and often patients cannot “get comfortable” and are restless or agitated. It is often associated with nausea and vomiting.
The diagnosis is usually made on imaging with a CTKUB and KUB x-ray, where the stone in the kidney or ureter is demonstrated. Often there is microscopic blood in the urine (haematuria).
If you have an associated infection or kidney function impairment on a blood test, you will usually be admitted for emergency treatment with a ureteric stent or percutaneous nephrostomy.

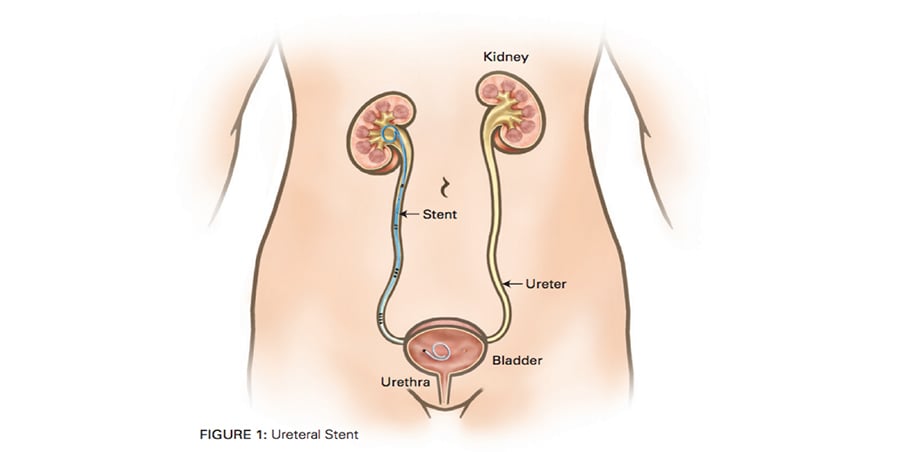
A ureteric stent is often offered for a stone impacted in the ureter when it is causing persistent pain, a large stone is unlikely to pass or there is an infection associated with the obstructed ureter.
The stent is placed at the time of the cystoscopy so there are no cuts. The stent is entirely internalised and unblocks the ureter. There is a curl in the kidney and another one in the bladder on either end of the stent to stop it from moving.
The stent will allow the kidney to drain and settle the swelling from the stone. It also helps the ureter to dilate so that in 1-2 weeks time, Dr Chong can pass a fine telescope (ureteroscope) up to the stone and fragment it under direct vision with a laser fibre.
We will outline options and suggest the best way to manage the stone depending on its size, location and your symptoms. Treatment options from least to most invasive include:
If your stone is small, particularly if it is less than 5mm, we may offer to see if it will pass by itself. Obviously your pain must be controlled with oral medications and you must otherwise be well. You will likely be placed on Tamsulosin to help the stone pass. It acts by relaxing the muscle in the lower end and tightest part of the ureter, to dilate it and increase the chance of stone passage. It is also the same medication that is used to treat men with an enlarged prostate (by also relaxing the muscles in the bladder neck and prostate).
A follow-up appointment in ~ 6-8 weeks will be organised with repeat scans to confirm that the stone has passed. If you like, you can also strain your urine to catch it, and this can be sent to the laboratory to be analysed to see what it is made of.
We may offer treatment if the stone has not passed or you experience problems while waiting.

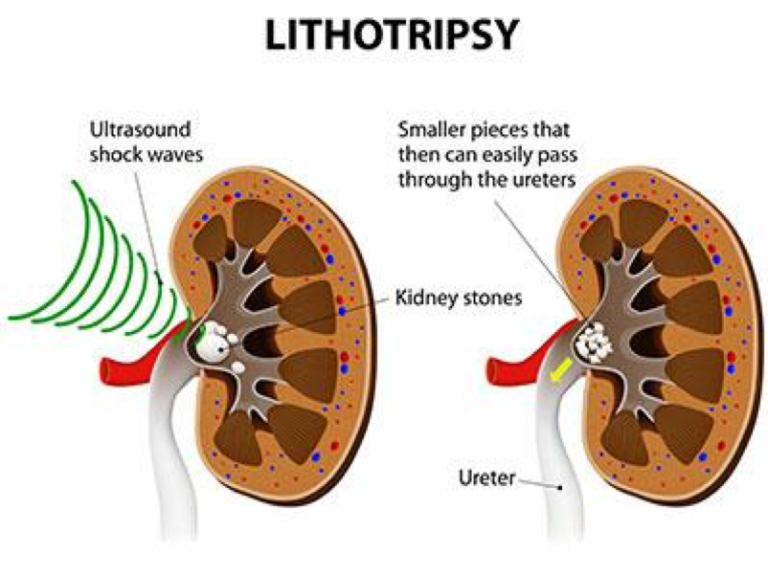
This is the least invasive treatment for a kidney stone as sound waves are focussed externally from the lower back onto the kidney stone under x-ray guidance. The stone then breaks up into smaller pieces that will hopefully pass naturally.
It is a day only procedure and the risks are usually minimal. Your surgeon will ensure you are not on blood thinners that may cause kidney bleeding. Otherwise, the main side effects are pain in the lower back where the ultrasound machine is applied.
Sometimes if the stone if very large or it does not break up into small pieces, the larger fragments may get caught in the ureter (steinstrasse) and require further treatment. That is why this treatment is best for stones less than around 10mm in the kidney.
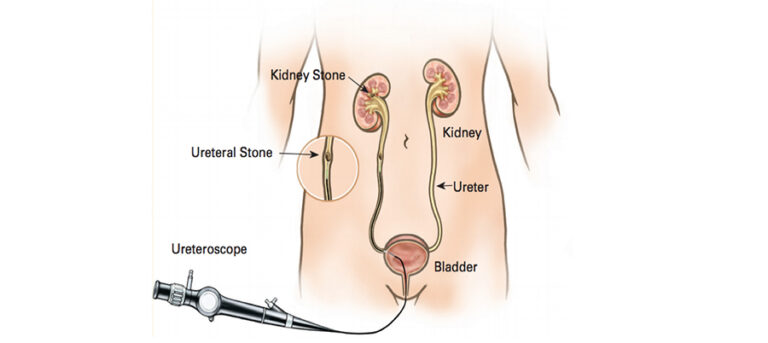
This is the commonest operation for stones in the ureter and kidney. A fine telescope can be passed through the urethra into the bladder, and then up into the ureter and kidney to directly visualise the stone. There a laser fibre is used to fragment the stone into fine dust particles which will pass.
A stent is usually placed at the end of the procedure to ensure that the ureter does not block immediately afterwards. It is usually removed 1-2 weeks later. If the ureter is very tight and does not allow the telescope to go up into the kidney, a stent will be placed. This will allow the ureter to dilate and then the telescope can be successfully passed into the kidney around a fortnight later.
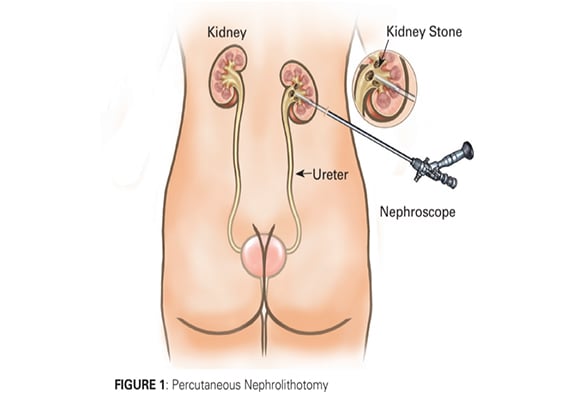
This is an uncommon operation offered to patients that have very large stones in their kidney. Due to the stone size, it is impractical to break the stone into fine particles to pass through the ureter. Instead, a hole is made in the flank to directly access the stone and break it into large pieces which are then pulled out. It is like “keyhole” surgery for large kidney stones.
A cystoscopy is initially performed so that x-ray dye can be injected up the ureter into the kidney (retrograde pyelogram). The patient is then positioned face down so that a needle can be punctured through the lower back into the kidney under x-ray guidance. The needle tract is dilated to around 1 cm so that a large telescope can be introduced into the kidney to directly visualise the stone, break in into pieces that can be pulled out through the tract.
A catheter is left in the bladder, ureter and the kidney (percutaneous nephrostostomy) and sequentially removed over the next few days. The goal is to debulk the stone although a flexible ureteroscopy may be required later to treat any smaller stone fragments that remain.
The majority of kidney stones are related to lifestyle issues. The two important changes that you can do to prevent stones are:
This is important for your health in general and will be re-iterated by you GP to prevent heart disease, stroke, kidney disease, diabetes, hypertension and high cholesterol.
In a small proportion of stone formers there is a metabolic predisposition to forming stones and Dr Chong will speak to you about how to treat it or may refer you to another specialist to treat the underlying problem. Examples include a high blood calcium level associated with an abnormality of the parathyroid gland. Also a high blood urate level, similar to how urate crystals form in joints in the condition of gout, can produce uric acid stones in the urinary tract. This can be prevented with a high fluid intake, Sodibic and Allopurinol.
Dr Chong is likely to organise follow-up in 6-12 months with repeat kidney imaging such as a renal ultrasound and KUB x-ray to ensure you are not forming any new stones that require treatment.
