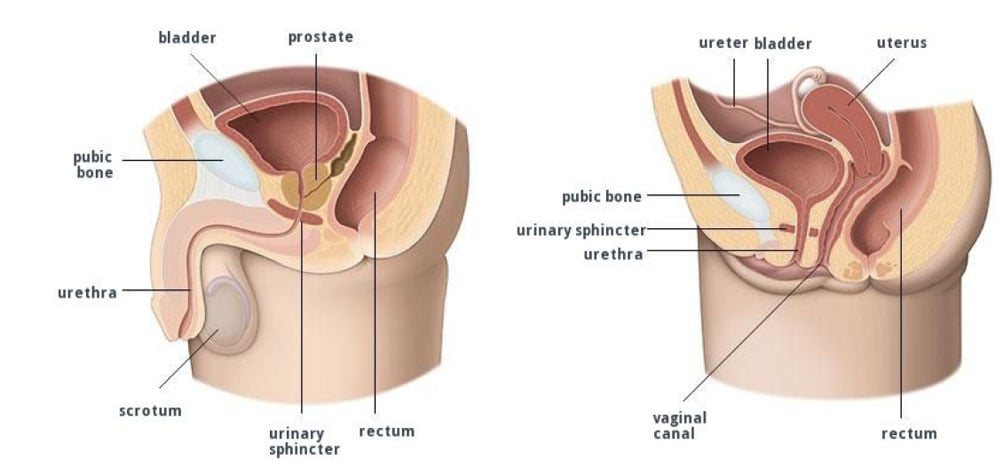
Lower urinary tract symptoms (LUTS) is a term used to describe a range of symptoms related to problems of the lower urinary tract including the bladder, prostate and urethra. LUTS affects both men and women, although usually for different reasons.
A uroflow and residual are usually performed as part of the initial assessment.